Sialorrhoea Management
Treatment is indicated when sialorrhoea is observed to have a negative impact on quality of life.29
Treating sialorrhoea requires a multidisciplinary team of specialists. This team should include paediatricians, behavioural therapists, speech and language pathologists, dentists, neurologists, paediatric otolaryngologists, social workers and coordinators.7
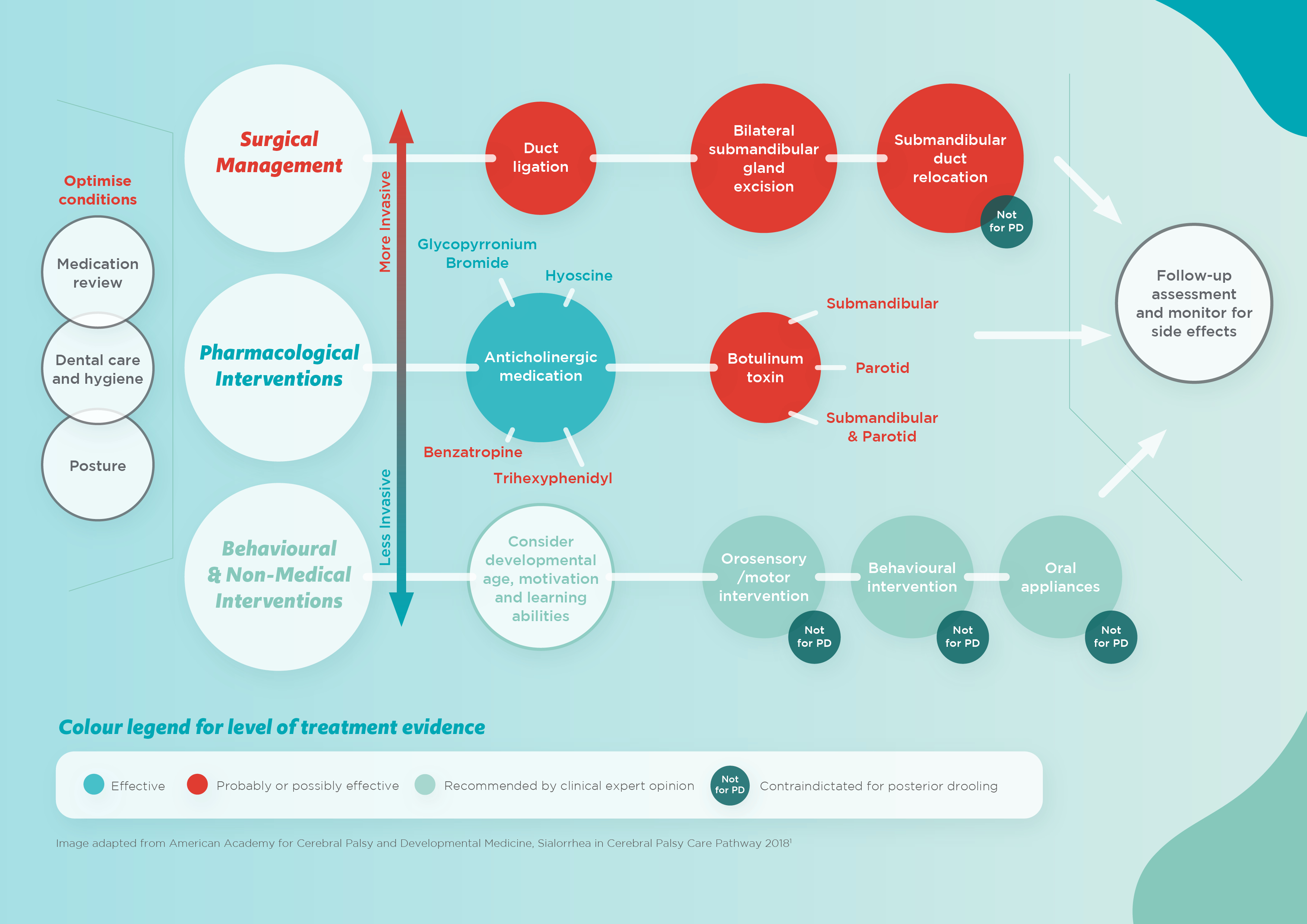
Sialorrhoea Care Pathway

Behavioural Interventions
The first step in the treatment of sialorrhoea is to optimise factors that may worsen the condition, such as oral health, postural control, medications and food and drink.1,5,13,19
Oral motor therapies and the use of oral appliances may be helpful, if appropriate for the child. Oral motor training aims to improve tongue mobility and closure of the lips and jaw.5,14 For oral motor therapies to be successful, adequate levels of cognition, concentration and motivation are required.13 Additionally, oral appliances may not be suitable for some children, for example, those with seizure disorders or severely limited control of tongue movement.1,13
Non-invasive approaches include oral facial facilitation with icing, brushing or vibration techniques. Additionally, behavioural modification techniques may be used, such as cueing, overcorrection, and positive or negative reinforcement.5,32
The evidence for management strategies is limited. They only work for a small number of children with mild to moderate drooling.1,10,13
Oral motor therapies and the use of oral appliances may be helpful, if appropriate for the child. Oral motor training aims to improve tongue mobility and closure of the lips and jaw.5,14 For oral motor therapies to be successful, adequate levels of cognition, concentration and motivation are required.13 Additionally, oral appliances may not be suitable for some children, for example, those with seizure disorders or severely limited control of tongue movement.1,13
Non-invasive approaches include oral facial facilitation with icing, brushing or vibration techniques. Additionally, behavioural modification techniques may be used, such as cueing, overcorrection, and positive or negative reinforcement.5,32
The evidence for management strategies is limited. They only work for a small number of children with mild to moderate drooling.1,10,13
Pharmacological Interventions
As saliva secretion is under parasympathetic autonomic control, largely dependent upon the activation of muscarinic receptors by acetylcholine, medications used in the management of sialorrhoea inhibit the actions of acetylcholine, thereby reducing saliva secretion.13,24 These include glycopyrronium bromide, hyoscine, benzatropine, trihexyphenidyl and botulinum toxin injections.1
Anti-muscarinic side effects of anticholinergics can include urinary retention, constipation, irritability, headache and blurred vision.1,13 Side effects should be discussed with the patient and parent/carer prior to treatment initiation.10
Anti-muscarinic side effects of anticholinergics can include urinary retention, constipation, irritability, headache and blurred vision.1,13 Side effects should be discussed with the patient and parent/carer prior to treatment initiation.10
Formulations
In children with neurological conditions, choosing a suitable formulation is just as important as choosing an appropriate treatment.
The selected formulation should support compliance, with minimum impact on lifestyle, and reduce the risk of medication errors. Attention should also be given to the ease of administration by the parent/caregiver.12

Surgical Interventions
Surgical interventions include sublingual or submandibular gland excision, duct ligation or submandibular duct relocation.1 Surgery may be indicated when behavioural and pharmacological interventions have proven ineffective or are unsuitable for the patient.14,21
Surgery can result in significant reduction of drooling with immediate results.5 However, this is the most invasive treatment option for sialorrhoea1,5 and some children only show temporary improvement with further physical and emotional impact.2,13 Such interventions are usually reserved for patients with profuse, persistent drooling with continued symptoms despite maximal conservative or pharmacological treatment.1
Rybrila is an oral solution of glycopyrronium bromide, suitable for use with feeding tubes, that is licensed for the symptomatic treatment of severe sialorrhoea in children and adolescents aged 3 years and older with chronic neurological disorders.9